


1Department of Dermatology, and 2Department of Clinical Pharmacology, Medical University of Vienna, Vienna, Austria
#These authors contributed equally and should be considered as first authors.
Various autoantibodies are detected more frequently in HIV-infected individuals than in HIV-negative controls; however, limited data exist regarding autoimmune blistering skin diseases. Using enzyme-linked immunoassay (ELISA) and indirect immunofluore-scence, no difference in the frequency and magnitude of autoantibodies against BP180, BP230, desmoglein 1 and 3 was found between 594 HIV-infected patients and 248 uninfected controls in this cross-sectional study (16.0% vs. 11.7%, respectively, for at least one positive ELISA, p = 0.11). Interestingly, reactive syphilis serology in both HIV-infected individuals and uninfected controls was associated with positive anti-BP180 ELISA results (adjusted odds ratio (OR) 2.14, 95% confidence interval (CI) 1.07–4.29, p = 0.03 and OR 4.70, CI 1.3–16.86; p = 0.0180). Our study shows a comparably low prevalence of cutaneous autoantibodies in both HIV-infected patients and uninfected controls lacking signs of autoimmune blistering skin disease. Positive BP180 ELISA in the absence of clinical signs of bullous pemphigoid should prompt further evaluation for syphilis antibodies.
Key words: HIV; autoimmune blistering skin disease; bullous pemphigoid; pemphigus; cART.
Accepted Jun 28, 2019; E-published Jul 8, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Christopher Schuster, Department of Dermatology, Medical University of Vienna, Waehringer Guertel 18–20, AT-1090 Vienna, Austria. E-mail: christopher.schuster@meduniwien.ac.at
The simultaneous occurrence of HIV-related immunodeficiency and autoimmune diseases is clearly documented. This cross-sectional study including 594 HIV-infected patients and 248 healthy controls lacking signs of autoimmune blistering skin diseases evaluated the frequency, titres and combinational appearance of autoantibodies directed against BP180, BP230, desmoglein 1 and 3, and showed no differences between the 2 patient groups. Interestingly, reactive syphilis serology in both HIV-infected individuals and uninfected controls was associated with positive anti-BP180 ELISA results, prompting a further evaluation for syphilis antibodies in patients with positive BP180 ELISA results and no clinical signs of bullous pemphigoid.
The spectrum of autoimmune phenomena in HIV-infected patients is unexpectedly broad and variable in the different stages of HIV infection and related to the immune system’s imbalances associated with the retroviral infection (1, 2). The likelihood of occurrence of autoimmune phenomena varies in the natural course of the HIV infection, but is particularly high in patients with a good immune status. As a consequence, the probability of autoimmune disease is highest after immune reconstitution due to combination antiretroviral therapy (cART). Recent developments, namely the international recommendation to treat all patients regardless of their CD4 count, will thus probably lead to a further increase in autoimmune phenomena in HIV-infected patients (3, 4). Indeed, this has recently been confirmed epidemiologically, showing a higher risk for certain autoimmune diseases, such as Sjögren syndrome or psoriasis, in HIV-infected patients compared with the general population (5, 6).
Autoimmune phenomena arise from various pathogenetic mechanisms, including molecular mimicry, dysregulation of the interaction between B and T lymphocytes, as well as relentless immunoactivation due to lifelong infection with HIV (7–9). In the sera of HIV-infected patients various autoantibodies, e.g. antinuclear antibodies, have been detected in higher frequency than in matched controls (10). Likewise, rheumatoid factor is found in every tenth HIV-infected patient (11), anti-neutrophilic antibodies in up to 42% (12, 13) and anti-cardiolipin antibodies in 36–67% (14). Of note, these autoantibodies are generally present at low titres and may have little, if any, clinical relevance.
In contrast to the abundance of data on rheumatological and haematological autoimmune diseases in HIV-infected patients, only limited data exist regarding autoimmune blistering skin diseases (15). In this heterogeneous group of acquired diseases blistering occurs after binding of autoantibodies to cutaneous antigens followed by the disruption of the highly complex structures involved in cell-cell and cell-matrix attachment (16, 17). When confronted with a potential case of autoimmune blistering skin disease, clinicians must interpret the results of various immunological assays in the context of the patient’s overall presentation. Routinely, 2 types of tests, namely indirect immunofluorescence (IIF) on monkey oesophagus and various enzyme-linked immunosorbent assays (ELISA), are now in common use as complementary tools in the screening and diagnosis of these rare diseases (18).
One small study performed in the pre-cART era look-ing for autoantibodies indicative of the most common autoimmune blistering skin disease, bullous pemphigoid, found that autoantibodies directed against the dermo–epidermal basement membrane proteins BP180 and BP230 were present in 38% of HIV-infected patients and were more common in later stages of HIV infection (15). So far, the frequency as well as combinational appearance of distinct cutaneous autoantibodies associated with pemphigus vulgaris (anti-desmoglein 1 and 3) and pemphigus foliaceus (exclusively anti-desmoglein 1) has not been studied in HIV-infected patients.
The aims of this study were to evaluate the frequency, titres, and combinational appearance of autoantibodies to cutaneous antigens associated with autoimmune blistering skin diseases in HIV-infected patients, and to guide clinicians when prescribing and analysing the results of antibody tests for autoimmune blistering skin diseases in HIV-infected patients.
Study population
In this cross-sectional study 594 HIV-infected patients and, as a control group, 248 persons requesting an HIV test or requiring post-exposure prophylaxis consultations at the HIV outpatient clinic of Vienna’s General Hospital were recruited between April 2017 and May 2018 using non-probability sampling. Neither group had any patient signs or symptoms indicative of autoimmune blistering skin diseases. All patients ≥18 years of age providing informed consent to participate were included in this study. The main exclusion criterion was pregnancy. The study complies with the Declaration of Helsinki, was reviewed and approved by the ethics committee of the Medical University of Vienna (ECS 1103/2017) and has been registered at Clinicaltrials.gov (identification number: NCT03129308).
Blood was sampled for the assessment of cutaneous autoantibodies during a routine venipuncture. Samples were centrifuged immediately thereafter and the sera were stored at –80°C until further processing. In HIV-infected patients various other parameters, including plasma HIV viral load, CD4+ T-cell count, hepatitis and syphilis serology, were routinely collected. Patients requesting an HIV test or requiring post-exposure prophylaxis consultations were additionally screened for hepatitis B surface antigen, hepatitis B and C antibodies and, depending on the exposure, syphilis antibodies (Venereal Disease Research Laboratory (VDRL) and Treponema pallidum particle agglutination (TPPA) tests).
Immunological assays
Circulating immunoglobulin G (IgG) antibodies against BP180 and BP230, desmoglein 1 and 3 (all Medical Biologicals Laboratories Co. Ltd, Nagoya, Japan) were detected using commercially available ELISA-kits according to the manufacturer’s instructions. IIF studies were performed on monkey oesophagus sections as previously described (Inova Diagnostics, CA, USA) (19). Briefly, patient sera were diluted at 1:10 and incubated on monkey oesophagus slides for 30 min at room temperature. Finally, antibody binding was visualized with a fluorescein isothiocyanate (FITC)-labelled goat anti-human IgG antibody (all INOVA Diagnostics, San Diego, CA, USA). To rule out the prozone effect, serial dilutions ranging from 1:10 to 1:160 were performed on 50 samples. The grading was performed by a single, blinded investigator throughout the entire study period to guarantee consistency of results. Four principal results in fluorescence studies were recognized: linear, intercellular, nuclear, and negative. For all patients with detectable anti-basement membrane antibodies in indirect immunofluorescence studies, further subclassification was carried out using the salt-split technique. Briefly, healthy adult skin collected after breast surgery was placed on 1 mol/l NaCl at 4°C for 24 h, embedded in optimum cutting tissue compound (Tissue-Tek, Sakura Finetek, The Netherlands), stored at –80°C until further processing, and subjected to the same staining procedures as described for IIF studies. All analyses for cutaneous autoantibodies described above were performed in an ISO-accredited facility (Department of Dermatology, Medical University of Vienna, Vienna, Austria) by experienced personnel.
Statistical methods
Continuous data were presented as median and interquartile range (IQR) and compared using Wilcoxon rank sum statistics. For the comparison of binary data, either a Pearson’s χ2 or Fisher’s exact test was used depending on the number of events. Spearman’s correlation coefficient was applied to assess the relationship between cutaneous autoantibodies and demographic and laboratory parameters. Next, univariate and multivariate logistic regression models were used to determine the relationship of various immunological, virological and demographic variables with positive cutaneous autoantibody ELISA and to calculate odds ratios (OR). ELISA and IIF results are available for all patients. Missing data for routine blood chemistry was < 5%. Syphilis antibodies were available in all HIV-infected patients and in 86% of uninfected controls. Two-sided p-values < 0.05 were used to indicate statistical significance. Stata 14.2 (College Station, TX, USA) was used for all analyses and graphs were drawn with GraphPad Prism version 5.03 (San Diego, CA, USA).
Study population
A total of 594 HIV-infected patients and 248 uninfected control patients met the inclusion criteria and were recruited. No patient had clinical signs or symptoms reminiscent of any autoimmune blistering skin disease. Detailed baseline characteristics of the patients at the time of diagnosis are presented in Table I.
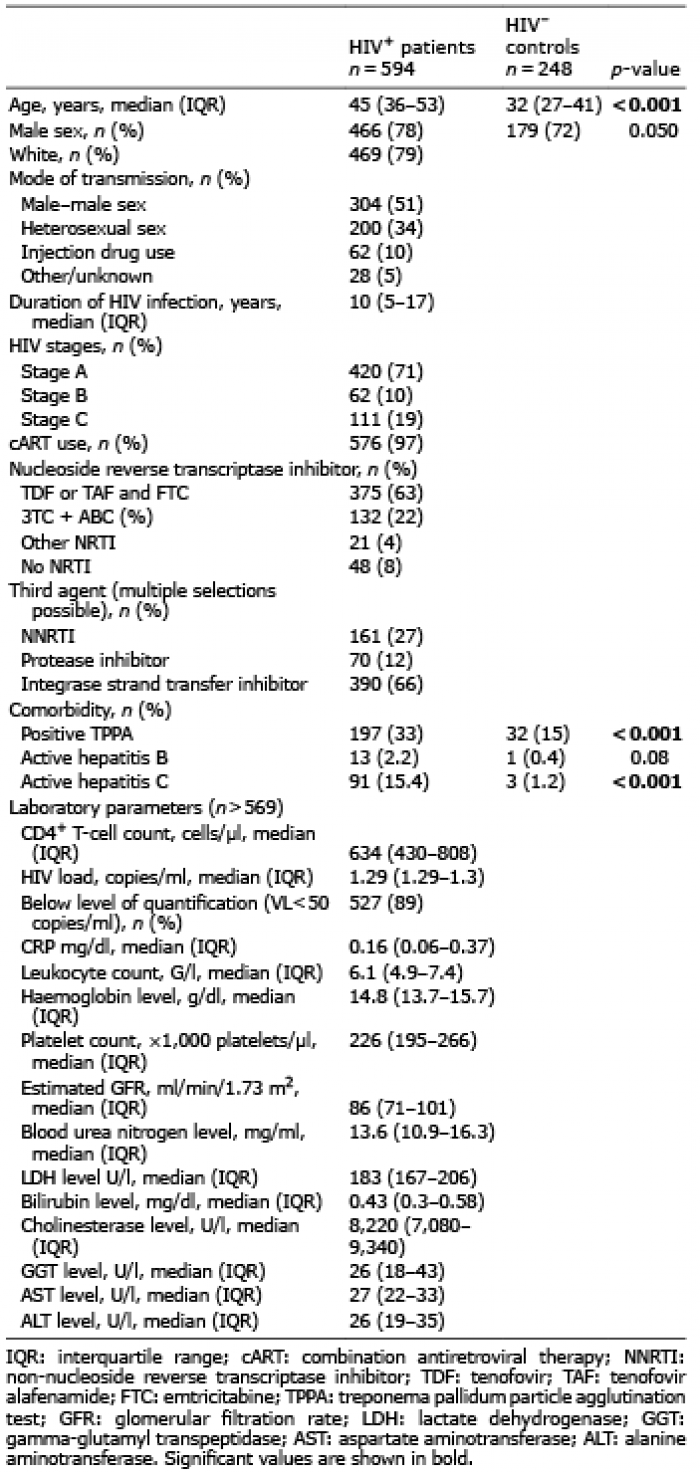
Table I. Baseline characteristics of the study and control populations
The median age of HIV-infected patients was 45 years, and the majority of infected patients were white (79%) and male (78%). The HIV infection was acquired primarily by homosexual (51%) or heterosexual intercourse (34%). Most patients were in CDC stage A (71%) and HIV-positive for 10 years (IQR 5–17). The median CD4+ T-cell count at study recruitment was 634 cells/µl (430–808) and 97% of infected patients received cART with a median HIV viral load of 1.29 (IQR 1.29–1.3) log10 copies/ml. Sexually transmitted diseases (STDs) were common with one-third of HIV-infected patients showing a reactive TPPA indicative of treated or active syphilis. Active hepatitis B and C were observed in 2.2% and 15.4%, respectively. The control group was also predominately male, younger with a median age of 32 years and exhibited a lower frequency of syphilis and hepatitis B and C coinfections (Table I).
Prevalence of cutaneous autoantibodies
Autoantibodies directed against BP180 and BP230 exceeding the upper normal range of 9 U/ml were found in 6.23% (37/594) and 5.72% (34/594) of HIV-infected patients, respectively, compared with 5.24% (13/248) and 4.03% (10/248) of controls (p = 0.58 and p = 0.32, Table II). Of note, only 8 patients displayed BP180 and BP230 double positivity with no statistical difference between the 2 groups (p = 0.78, Fig. 1a). Further subclassification of all BP180- and BP230-reactive sera using the salt-split technique on human skin showed exclusively negative results with the exception of one HIV-uninfected individual with a positive BP230 ELISA and a linear signal on the epidermal side. In univariate and multivariate logistic regression models, positive BP180 ELISA results were only predicted by the concomitant presence of a nuclear staining in IIF (adjusted OR (aOR) 3.18, p = 0.008) and reactive TPPA (aOR 2.14, p = 0.03). Interestingly, various demographic, HIV- or infection-related markers were not associated with positive BP180 results (Table SI). In uninfected controls, however, only reactive TPPA (aOR 4.7, p = 0.018) was associated with positive BP180 ELISA results (Table SII). Surprisingly, the same models were unable to predict positive BP230 ELISA (data not shown).
Similar to the bullous pemphigoid autoantibodies, no difference in frequency was observed with the pemphigus autoantibodies against desmoglein 1 and 3 (Fig. 1b, Table II). Positive results for both desmoglein 1 and 3 were found in less than 1% in either group. A total of 63 patients exhibited a low titre intercellular signal in IIF, yet only 2 of these patients were positive for either desmoglein 1 or 3 (Fig. 1b, green circle). Interestingly, twice as many controls than HIV-infected patients showed a low-titre intercellular staining pattern in IIF studies (12.1% vs. 5.56%; p = 0.001) and no correlation was found between results from ELISA and IIF (r = –0.029, p = 0.40 for desmoglein 1 and r = –0.001, p = 0.80 for desmoglein 3) as well.
Table II. Comparison of results from enzyme- linked immunoassay (ELISA) and indirect immunofluorescence of the study and control populations
Fig. 1. Dot plots show the autoantibody levels (a) against BP180 and BP230 or (b) desmoglein 1 and 3 in HIV-infected patients (red circles, n = 594) or uninfected controls (black circles, n = 248). Grey lines mark the upper normal value (9 U/ml for BP180 and BP230 and 20 U/ml for desmoglein 1 and 3). Each dot represents one patient. Green circles indicate patients with positive enzyme-linked immunoassay (ELISA) results and corresponding positive indirect immunofluorescence signal.
This study investigated the prevalence of cutaneous autoantibodies in HIV-infected patients, demonstrating that their frequency is similar to uninfected controls.
A previous report originating in the pre-cART era applying Western blotting noted that 38% of HIV-infected patients showed circulating bullous pemphigoid antibodies and that the frequency of autoantibodies was dependent on the duration of the HIV infection, increasing from 21% in early HIV infection to approximately 40% in later stages of infections (15). Using more sensitive and specific techniques, namely ELISAs targeting the relevant pathogenetic recombinant proteins, we found a lower frequency of autoantibodies directed against BP180 and BP230 in HIV-infected and uninfected controls, being within the range of what has previously been described in healthy populations (20). This finding is all the more surprising given that the median age of uninfected controls was more than 10 years lower than that of HIV-infected patients and age being the most important risk factor for the development of bullous pemphigoid (16, 21, 22). Only the presence of TPPA antibodies and the presence of nuclear staining in IIF, but not a single demographic, HIV or infectious laboratory marker, predicts the magnitude of, or positivity for, BP180 autoantibodies in HIV-infected patients using univariate and multivariate statistical modelling. One possible explanation for the association between BP180 autoantibodies and reactive TPPA is the extracutaneous expression of BP180 in tissues, such as the brain (23). It is possible that neuroinflammation in the course of syphilis elicits an (auto)immune response, leading to cross-reaction between neural and cutaneous antigens, eventually leading to the formation of BP180 autoantibodies. The absence of the epithelial isoform of BP230 (24), desmoglein 1 and 3 in nerve tissues would corroborate this notion.
The lower prevalence of bullous pemphigoid autoantibodies in HIV-infected patients is in contrast to the study results found in the pre-cART era by Kinloch-de Loës et al. (15) and may reflect the high frequency of suppression of viral replication with subsequent immune reconstitution by cART in our cohort. In line with this, it has been recently shown that the prevalence of antineutrophil cytoplasmic antibodies (ANCAs) and anti-cardiolipin antibodies is nowadays lower than in previous studies, which has also been attributed to the effects of cART (10, 25, 26). In total, these findings support the notion that cART-induced immune-reconstitution and the reversal of systemic inflammation in HIV-infected patients may also reverse the risk to develop autoantibodies to cutaneous antigens to levels observed in healthy controls (9). An alternative explanation for the higher frequency of autoantibodies directed against the hemidesmosomal antigens BP180 and BP230 in the study performed in the pre-cART era might be the presence of autoantibodies recognizing epitopes lying outside the pathogenetically relevant NC16A domain, thus hinting at a negligible clinical relevance (27, 28). Theoretically, it is also possible that the rate of positive ELISA results is attributed to an excessively low cut-off value (29, 30). Indeed, most patients with positive ELISA results had only slightly or moderately elevated values, although some patients, especially HIV-infected ones, also showed high titres (see Fig 1a).
Interestingly, positive results in BP180 and BP230 ELISA did not translate into the expected linear staining pattern in IIF studies on monkey oesophagus in both HIV-infected and uninfected patients. Likewise, of those patients with positive BP180 or BP230 results, the vast majority showed negative results using salt-split analyses on human skin. This same discrepancy has also been observed in patients with Alzheimer’s disease whose anti-BP180 positive sera lacked reactivity with IIF, but instead recognized tyrosine-hydroxylase-positive neurones in human and rat substantia nigra (31, 32). It remains to be elucidated why BP180 autoantibodies of patients with Alzheimer’s disease or HIV infection, as well as a substantial fraction of uninfected controls, do not bind to the cutaneous basement membrane. An alternative, technical explanation for this discrepancy might be the higher sensitivity of ELISA relative to immunofluorescence studies or the use of monkey oesophagus as substrate instead of human skin (29).
On the other hand, 20 out of 21 patients with weak linear signals in IIF were negative for BP180 and BP230 ELISA. This negativity might also underscore the fact that none of the patients had clinical signs of autoimmune blistering skin disease and might be related to the visualization of pathogenetically irrelevant autoantibodies (33). Similar to the situation with the bullous pemphigoid autoantibodies, no statistical difference was observed in the frequency of autoantibodies directed against desmoglein 1 and 3. Of note and unexpectedly, in IIF studies uninfected controls showed a higher prevalence of anti-nuclear and intercellular staining than HIV-infected patients.
For various autoimmune blistering skin diseases, ELISA values and corresponding IIF titres are used as laboratory surrogates for the disease activity or severity (19). Despite detecting autoantibody levels comparable to those seen in patients with extensive bullous pemphigoid or pemphigus disease in a few HIV-infected patients, none of our patients displayed any symptom or sign indicative of autoimmune blistering skin disease. Of note, head-to-head comparisons of sera with strongly elevated autoantibody levels with immunofluorescence studies were mostly discordant and not showing the expected pattern in IIF (arrows in Fig. 1a, b). On the other hand, low-titre signals in IIF lacking corresponding positive results in ELISA might be due to visualization of pathogenetically irrelevant autoantibodies (33).
In general, the overall significance of positive ELISA against immunodominant cutaneous epitopes in patients without signs and symptoms of autoimmune blistering skin disease is currently unknown. It is possible that the chosen cut-off values could have been too low, thus leading to an excess rate of false-positive results (29, 30). However, it is also possible that the formation of autoantibodies against cutaneous antigens represents an early stage of the development of autoimmune blistering skin disease and it remains to be investigated whether the increased genetic susceptibility observed in patients with the HLA-DQβ1*0301 allele with bullous pemphigoid is also found in HIV-positive patients with detectable autoantibodies (34).
The high number of study participants relative to most other studies, together with the inclusion of various variables allowing statistical adjustment, as well as the control arm, represent strengths of this study. One major limitation of this study is its cross-sectional design, as it is not possible to determine the temporal relationship between the HIV infection and the development of cutaneous autoantibodies. Although we cannot exclude a selection bias, the high participation of up to 40% of our entire HIV cohort speaks for a balanced recruitment.
Taken together, this study shows a comparably low prevalence of cutaneous autoantibodies in both HIV-infected patients and uninfected controls lacking signs of autoimmune blistering skin disease. Positive BP180 ELISA in patients lacking typical clinical signs of bullous pemphigoid should prompt further evaluation for syphilis and antinuclear antibodies.
The authors thank Tina Holper for her invaluable technical assistance and Regina Aichwalder, Renate Eder, Manuel Kleinrath, Silvia Kovar, Manuela Lenk and Helmut Stranzl for their continuous support.
This work was supported by a research grant of the Austrian Science Fund (KLI716-B30) and the Austrian AIDS Society to C.S.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize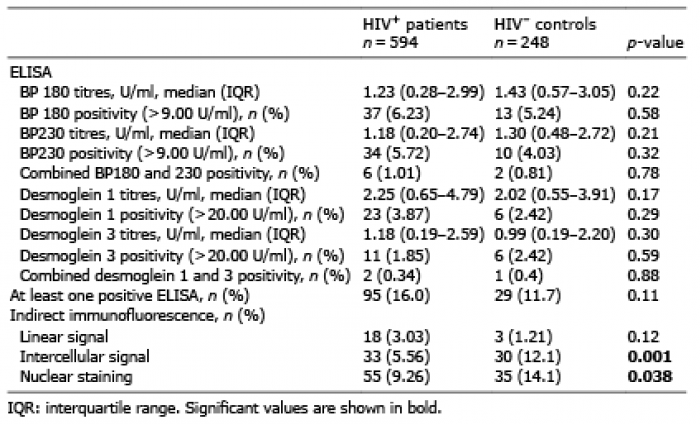 Click to show fullsize
Click to show fullsize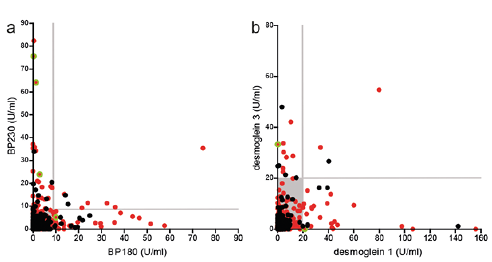 Click to show fullsize
Click to show fullsize